Our Services - Paediatric Eye Diseases and Strabismus
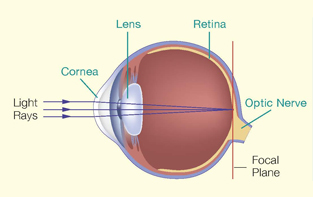
Normal
Short-sightedness
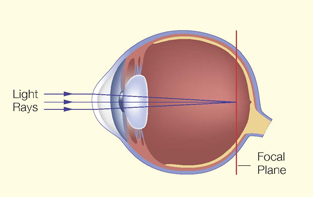
Short-sightedness (myopia) is the most common eye problem in the world. This phenomenon is even more prominent in Hong Kong. Studies show that 30 to 70% of primary school children in Hong Kong suffer from short-sightedness.
Short-sightedness is usually due to elongation of the eyeball. Thus, the object is focused in front of the retina. A child with short-sightedness typically complains of blurry vision for distant objects, but is less so when seeing near objects. The child will have difficulty in reading the blackboard and he might also squint his eyes when looking at distant objects.
Long-sightedness
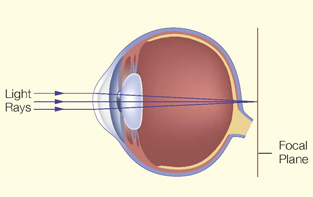
Long-sightedness (hypermetropia or hyperopia) is less common than short-sightedness amongst Hong Kong children. Long-sightedness is due to relatively short eyeball.
The symptoms of long-sightedness are less obvious than short-sightedness. If a child only has mild longsightedness (less than 2D or 200 degrees), the elasticity of his lens helps to keep things in focus and he or she can see rather clearly. However, if the child has severe longsightedness, he or she will have difficulty in focusing and thus will see poorly. The child may even develop squint (strabismus) and lazy eye. Under these circumstances, the child must wear glasses.
Astigmatism
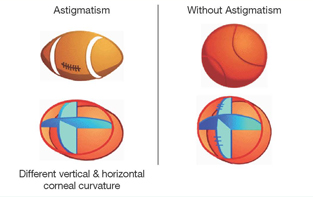
In astigmatism, the curvature of the cornea is different along different axes. As a result, light rays entering the eye are focused at different points instead of a single point. This will create a blurry image. The child may suffer from eyestrain. He may squint his eyes or adopt a head tilt. A child with high astigmatism requires glasses.
Prevention of Progression of Short-sightedness
While wearing spectacles or contact lenses can improve vision for children with short-sightedness, both methods may cause inconvenience and wearing contact lens may even give rise to complications.
High myopia is associated with higher chance of eye diseases, such as retinal detachment, macula haemorrhage, cataract and glaucoma etc.
The causes of short-sightedness are still unknown, so are those of short-sightedness progression. Both genetic and environmental factors play a role. Shortsightedness progression is more significant in children between 6-12 years old.
Atropine eye drops
Studies on the effectiveness of atropine eye drops (0.5 to 1.0%) in reducing short-sightedness progression started as early as in the 70s. Atropine is a non-selective anti-muscarinic blocker. It can inhibit excessive scleral growth and thus reduce or arrest short-sightedness progression. Studies showed that 0.5% and 1.0% atropine eye drops can slow short-sightedness progression by 75% and 80% respectively. On the other hand, atropine will cause pupil dilation and inhibit accommodation (zooming of focus to see near things), causing photophobia (light sensitivity) or blurry vision when seeing near objects. Photochromatic and progressive lenses may hence be required in children using atropine eye drops.
Recent studies showed that using lower concentration of atropine eyedrops (0.01 to 0.1%) can slow shortsightedness progression with less side effects. Atropine (0.01%) can reduce progression by 60%, but the average increase in pupil dilation is only about 1mm and 95% of children do not require progressive lenses for near vision.
In summary, topical atropine can slow down shortsightedness progression in children. However, its application has to be considered on individual basis. Regular monitoring is needed when using the eyedrops.
Can progressive lens arrest or reduce short-sightedness progression?
One of the hypotheses of preventing short-sightedness progression is to control accommodation. Progressive lens is a specially designed lens to achieve this purpose. A progressive lens is a one-piece lens whose shortsightedness power varies gradually from a highest value in the upper portion to a lowest value in the lower portion. The child is asked to use the upper portion for viewing distant objects and the lower portion for nearer objects. However, the evidence for arresting or preventing shortsightedness progression by progressive lens is very weak and not well established.
Can contact lens arrest or reduce short-sightedness progression? Some studies found that there was no difference in shortsightedness progression between children wearing Rigid Gas Permeable (RGP) lens and those wearing spectacles.
Orthokeratology (Ortho-K, OK lens), which was introduced in the 70s, uses tight-fitting, flat, rigid contact lenses to decrease the curvature and refractive power of the cornea. Lenses are changed periodically to progressively flatter ones. After the cornea has been sufficiently flattened, retainer lenses are usually worn at night to preserve the modified shape, otherwise the eye will revert back to the original corneal curvature and refraction. Parents must be aware that there are potential risks associated with contact lens wearing, such as corneal abrasion, ulcer and infection, leading to permanent loss of vision.
Strabismus (Squint)
Strabismus (squint) is a condition in which the eyes are misaligned. The two eyes point towards different directions. One eye is fixed at the object of interest, while the other eye is misaligned to a different direction. The misaligned eye may be directed inward (convergent squint), outward (divergent squint) or upward (vertical squint).
A child with squint will only use the properly aligned eye to see. The image from the misaligned eye will be suppressed. This will lead to loss of binocular vision and may even cause lazy eye. Squint also causes a cosmetic problem that will affect the child's self-esteem.
In most cases, squint is caused by improper eye muscle balance. However, in a small number of children, squint is caused by serious underlying eye diseases such as congenital cataract, cancer of the eye, etc. Therefore, we should never neglect a squint.
Treatment of squint includes glasses, patching, vision training and surgery. Some people have a misconception that children will outgrow their squint. Actually these people have confused true squint with pseudo squint. In a child with pseudo squint, his eyes are actually normal and are well aligned. He has a wide and flat nose bridge which gives the illusionary appearance of crossed eyes. As he grows older and the nasal bridge becomes higher, this illusionary appearance of crossed eyes will disappear. However, in a child with true squint, his eyes are misaligned. This condition will not outgrow. He needs early treatment to straighten the eyes and allow normal vision to develop.

Convergent Squint

Divergent Squint

Vertical Squint

Head Tilt Caused by
Vertical Squint
Lazy Eye (Amblyopia)
During the first 8 years of life, the visual system is in a developmental stage. Though a newborn infant is able to see, his vision will continue to develop with proper use of his eyes. If proper use of his eye is hindered, the vision of that eye will not develop properly, and that eye will become a lazy eye. A lazy eye has poor vision and is not correctable with glasses.
The reasons that hinder visual development include firstly, misaligned eyes. Secondly, it could occur when one eye is out of focus with respect to the other because of a stronger degree of short-sightedness, long-sightedness or astigmatism. The more out-of-focus eye “turns off” and becomes lazy. Thirdly, droopy eyelid and eye diseases like cataract that inhibit light from entering the eye also lead to lazy eye.

Droopy Eyelid

Congenital Cataract
Lazy eye commonly occurs in only one eye of a child. Parents might not be aware that their child is only seeing the world with one eye unless they bring their child for a formal eye examination. If lazy eye is detected in early childhood, it can be corrected by patching the normal eye. However, after the age of eight, lazy eye becomes irreversible.

Treatment of Lazy Eye with Occlusion

Normal Vision

Amblyopic Vision
Eye Examination
A young child will not be able to tell you of his visual problems. Therefore, parents should bring their child for a comprehensive eye examination. A comprehensive eye examination can tell you whether the child has short-sightedness, long-sightedness, astigmatism, squint, lazy eye or any other eye diseases. If an abnormality is detected, early treatment can be offered. If the eyes are found to be normal, this would be a piece of useful baseline information for future reference.
An eye doctor is able to examine a child of any age and also check whether the child has focusing problems. For infants, the eye doctor might need to use special techniques, instruments or diagnostic eye drops.
Children should have annual comprehensive eye examination after the age of 4. Eye examination is paramount importance if you notice following conditions in your children:
- An infant who has abnormal visual response. For example, he does not respond to light or follow toys and cannot recognize the face of his parents.
- The eyes have abnormal external appearance (e.g. droopy eyelids, redness and swelling of the eyes, bulging eyeballs, or white reflex from the pupils, etc.)
- Frequent tearing, blinking and rubbing of eyes.
- Blurred vision, double vision.
- Abnormal alignment of eyes, e.g. eye turned inward, outward or upward.
- Head tilt when looking at objects.
- Squinting of eyes when looking at objects or when copying from the board.
- Any other condition that makes you worried.

Squint Assessment

Assessment of Stereopsis